
Introduction
Athletes train daily at a high intensity in attempt to achieve their best performance in competitions. High-intensity training has been reported to improve the physical ability of athletes in terms of aerobic capacity, high-intensity running ability, and body mass index; however, it can also increase the frequency of injuries and illnesses [1]. Because these negative outcomes arising from high-intensity training can lower athletesŌĆÖ performance and affect the success of individual athletes or their teams [2,3], it is important to monitor the condition of the athlete and prevent injuries and illnesses.
An athleteŌĆÖs condition consists of many factors, such as physical, environmental, and psychological factors. Among these factors, pain, a physical factor, has been reported to give rise to physical problems experienced by many athletes [4]. In addition, pain is an initial symptom of many types of injuries, and continuing to participate in training while experiencing pain may cause a decrease in performance, making it impossible to participate in training, further leading to more serious injuries over time (time loss injury) [5]. Thus, a greater understanding of pain experienced by athletes is important to injury prevention.
Handball is a high-intensity contact sport. In previous studies, high incidence rates of injuries were reported regardless of athlete age and level of competitiveness in handball [6-9]. Engebretsen et al. reported that handball had the highest injury risk in team sports tournaments during the 2004 Olympic Games [6]. Moreover, studies that targeted young handball players showed that the incidence of injury is as high as the senior level [7]. In contrast, pain that is not reached time-loss injury has been investigated by several studies. According to a study investigating symptoms from problem elbows for goalkeepers, more than 80% of all players reported that they had elbow pain in the present or the past [10]. In addition, the study on shoulder pain for female handball players reported that more than 50% of players had pain in the present or the past [11]. However, studies on pain normally specialized in some body parts, the actual extent of pain occurrences, which are the initial symptoms of many injuries, have not been adequately studied. Moreover, several studies have investigated the relationship between training load (physical load) and injuries in handball, and the frequency and body part of injury have been reported to vary by training period, which is determined by the amount of training and training type [12]. Further, M├Ėller et al. demonstrated that a rapid increase in physical load increases the risk of shoulder injury in elite youth handball players [13]. However, the relationship between pain occurrence and changing daily physical load remains poorly understood. It is believed that clarifying these factors will help prevent injuries and facilitate conditioning throughout the season. Therefore, the purpose of this study was to clarify the actual extent of pain occurrences experienced by athletes and to examine the relationship between pain and physical load. We hypothesize based on a 12-month prospective cohort study that the degree of pain occurrence is related to an athleteŌĆÖs physical load and that the frequency and body part of pain vary with changes in physical load.
Methods
Subjects
Fourteen female handball players belonging to a university handball team participated in this study. Three of them did not complete the entire training because of injuries at the start of the study and who underwent rehabilitation for most of the investigation period were excluded. Therefore, the subjects were 11 female handball players (average age: 19.5 ┬▒ 0.7 years, average height: 164.0 ┬▒ 4.9 cm, average weight: 59.4 ┬▒ 6.1 kg, average years of handball experience: 8.0 ┬▒ 2.7 years). This team has a track record of winning at the All Japan Student Handball Championships, and each had a high level of skill and handball experience. This study was conducted with the approval of the university ethics committee (no.25-74), and informed written consent to participate in this study was obtained from each participant.
Procedures
We conducted a prospective cohort study to investigate pain occurrences, handball playing hours, and types of matches and training during the 12-month period from October 1, 2012, to September 30, 2013. The participants took part in daily handball matches and training planned by their head coach and responded to a questionnaire on pain.
Pain Surveillance
Pain was defined as ŌĆ£pain caused by participation in a handball match or training.ŌĆØ Using the questionnaire, participants themselves described their pain experience every day. The questionnaire consisted of two items: body regions and a corresponding pain severity score. Pain severity scores consisted of a 6-point scale, with a score of 1 indicating the mildest pain and a score of 6 indicating the most severe pain (Table 1). If a player was unable to take a full part in match or training due to injury (time loss injury), the pain that occurred during that period was excluded from the analysis. To grasp the nature of pain experienced each day by the participants, all pain that occurred was counted as one case of pain. For example, if pain was experienced at two different body regions on the same day (e.g., shoulder pain and ankle pain), this was counted as two pains.
Physical load on handball
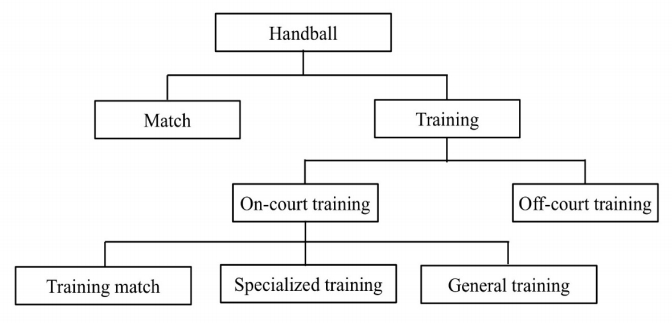
Physical load on handball was defined as ŌĆ£amount of playing hours of handball match and training.ŌĆØ Using a video camera, we recorded the playing hours and types of matches and training each day for each participant. The types of physical load were classified into seven categories by the chief investigator and head coach (Figure 1) [12]. In handball, official matches such as league matches and tournaments were designated as ŌĆ£match,ŌĆØ and others were designated as ŌĆ£training.ŌĆØ With respect to training, we classified practices on the handball court as ŌĆ£on-court trainingŌĆØ and practices outside the handball court as ŌĆ£off-court training.ŌĆØ In addition, with respect to oncourt training, practice games under official rules is called ŌĆ£training match,ŌĆØ practices specialized for handball other than training match were called ŌĆ£specialized training,ŌĆØ and practices not related to handball such as dashing, stretching, and other types of ball games were taken as ŌĆ£general training.ŌĆØ The total physical load calculated for each participant and physical load for each category were summed for all participants daily.
Statistical methods
The incidence rate of pain (1000 player hours) obtained by dividing the number of pain occurrences by exposure (playing hours) was calculated and expressed with a 95% confidence interval (95%CI) [14]. To determine the relationship between pain and physical load, SpearmanŌĆÖs correlation coefficient was used for the number of pains daily and physical load. The correlation coefficients were defined as follows: very weak, 0 Ōēż | rs| Ōēż 0.20; weak, 0.21 Ōēż | rs| Ōēż 0.40; moderate, 0.41 Ōēż | rs| Ōēż 0.70; strong, 0.71 Ōēż | rs| Ōēż 0.90; and very strong, 0.91 Ōēż | rs| Ōēż 1.00 [15,16]. The levels of significance for each item analyzed via SpearmanŌĆÖs correlation coefficient were adjusted using the false discovery rate (FDR) [17]. SPSS Statistics software version 24.0 was used for all statistical analyses, and the level of statistical significance was set at p=0.05.
Results
Pain
Over the course of the 12-month survey, the total playing hours was 5893.6 hours, of which the match was 206.5 hours (24 days) and the training was 5687.1 hours (252 days). The total number of pains was 1698, the pain incidence rate was 288.1 pains per 1000 player hours (95% CI: 274.4-301.8). The characteristics of pain are described in Table 2 to Table 4. In terms of body regions, the ankle (n=311, 18.3%) was the most common, followed by the lower back (n=226, 13.3%), foot (n=218, 12.8%), Achilles tendon (n=157, 9.2%), and thigh (n=151, 8.9%). With regard to the score, score of 2 (n=751, 44.2%) was the most common, followed by 3 (n=331, 19.5%) and 5 (n=326, 19.2%). In terms of pain severity scores by body regions, score of 5 was the most frequent for the elbow (n=83, 67.5%), sternum/ribs/upper back (n=18, 60.0%), and foot (n=91, 41.7%) and score of 2 was the most common for other parts.
Physical load on handball
Table 5 shows the physical load over the 12-month period. During the study period, the overall physical load was 5893.6 hours, of which matches comprised 206.5 hours (3.5%) and training comprised 5687.1 hours (96.5%). Average daily physical load was 16.2 hours in overall physical load, and 0.6 hours in match and 15.6 hours in training. For training, oncourt training was 4431.6 hours (77.9%) and off-court training was 1255.5 hours (22.1%). In terms of average daily physical load, on-court training was 12.1 hours and off-court training was 3.4 hours. In addition, during on-court training, the training match was 894.7 hours (20.2%), specialized training was 2798.7 hours (63.2%), and general training was 738.3 hours (16.7%). Average daily physical load was 2.5 hours in training match, 7.7 hours in specialized training, and 2.0 hours in general training.
Relationship between pain and physical load
Table 6 shows the relationship (correlation coefficient) between the number of pain occurrences per day and physical load. Significant moderate correlations were observed between handball (rs=0.657), training (rs=0.626), on-court training (rs=0.591), specialized training (rs=0.588) and overall pain occurrences. In addition, significant weak correlations were observed between overall pain occurrences and training match (rs=0.356) and general training (rs=0.364). For body regions, in the ankle, significant moderate correlations were observed between handball (rs=0.504), training (rs=0.481), on-court training (rs=0.499), and specialized training (rs=0.510), and significant weak correlations were observed between training match (rs=0.230) and general training (rs=0.396). Significant moderate correlations were observed between the lower back and handball (rs=0.433) and training (rs=0.410); significant weak correlations were observed between on-court training (rs=0.342), specialized training (rs =0.378), and general training (rs=0.227). Moreover, significant weak correlations were observed between foot and handball (rs=0.222) and specialized training (rs=0.210).
Discussion
Over the course of this 12-month prospective cohort study in female university handball team, many pain symptoms occurred, and it became clear that athletes continue to compete in games despite experiencing pain. In addition, pain occurrence was found to be related to physical load, indicating a relationship with on-court training in particular. Furthermore, the types of physical load differ by body region of pain occurrence.
The overall pain incidence rate was 288.1 pains/1000 player hours. This incidence rate is high and it is clear that many handball players continue playing despite experiencing pain, which was not captured through handball injury surveys. The injury definition of ŌĆ£medical attentionŌĆØ and/or ŌĆ£time lossŌĆØ was used when recording injuries in injury surveys. Medical attention injury is an injury that results in a player receiving medical attention by a qualified medical practitioner, and time loss injury is an injury that results in a player being unable to completely participate in future training or match play [18]. Therefore, pain that does not require medical attention or does not result in time loss is not recorded in these injury surveys.
With regard to body regions, the ankle was the most frequently affected body part, followed by the lower back and foot. In the handball injury survey, the ankle is the main body region where injury commonly occurs [19-21]. As the body regions in this study were also similar, it can be said that ankle injuries and pains are inherent in handball. Previous studies have reported that the lower back is one of the body parts where overuse injury often occurs in handball [7,22,23]. According to a 13-week injury survey study targeting elite Norwegian handball players, 12% of all players had physical problems including pain in the lower back throughout the study period. It was reported that the prevalence rates of lower back problems, as well as knee and shoulder problem were high [23].
By looking at pain severity based on the severity score, approximately half of the cases had a score of ŌĆ£2,ŌĆØ which describes pain but not of a degree that affect performance, with respect to overall pain occurrence. From this, we believe that it is important to prevent mild pain from progressing to pain that may affect an athleteŌĆÖs performance (score of 3 or higher in this study). In contrast, 40% (score3-6) of overall pain occurrence affected the performance. Among them, it became clear that 53.3% of the pain (score4-6) always restricted the athleteŌĆÖs performance. In terms of body regions, score of 5 was the most common at the elbow, sternum/ribs/upper back, and foot and score of 2 was the most common for other parts. In particular, elbow pain with a score of 5 accounted for 67.5%. An epidemiological study concerning elbow problems in handball shows that roughly 30% of field player have elbow problems such as pain in the past and/ or present [24]. Moreover, the main mechanism of elbow problems for field players is repetitive overhead throwing, mainly in the throwing arm. As approximately two-thirds were severe pain (score of 5), future study is needed to investigate further the mechanism.
In relation to pain occurrence and physical load, the overall pain occurrence was related to physical load, in which moderate or weak correlations were observed with respect to all categories in on-court training. This indicates that when the daily number of pain occurrences and physical load are observed over time, the number of pain episodes increases as the number of on-court training hours increase. In terms of body regions, the ankle and thigh also exhibited the same tendencies and correlated with all categories with respect to on-court training. In addition, the lower back had weak correlations with specialized training and general training. By contrast, pain occurrences in the foot and Achilles tendon were low and correlated only with specialized training among on-court training. Based on these results, it is necessary to introduce preventive measures that incorporate changes in physical loads because the relevant categories differ depending on the body parts that experience pain.
The present studyŌĆÖs major strength is that it investigated the actual extent of pain occurrences experienced by athletes which are not captured in handball injury surveys. However, there are some limitations in this study. The primary limitation was the small number of participants. As we used paper questionnaire as medium to capture pain occurrence and video camera to measure physical load, the investigator had to distribute the questionnaire and record handball match and training every day. For this reason, the participants were only from one handball team. Therefore, findings in this study may be applicable only to university female handball team. Future studies are needed to improve our methodological approach, for example use of web-based questionnaire, and to include sufficient sample size.
Another limitation was that we investigated only the body part and severity score in the whole body by self-reported questionnaire in pain occurrence. Thus, the mechanism and pathology of pain are not yet clear. Information about the type of movement or activity in which the pain occurred is important when introducing preventative measures. In addition, subjective pain was investigated using a self-reported questionnaire in previous studies of pain in handball [10,11]. According to the definition of International Association for the Study of Pain, pain is defined as an unpleasant sensory and emotional experience and is always subjective [25]. Based on the results of these previous studies, we subjectively assessed the pain that handball players experienced. However, it is important for pain and injury prevention to understand both subjective pain and the pathology of pain objectively. Furthermore, it was revealed that overuse injuries in handball frequently occur in the lower back and shoulder. Overuse injuries usually start with mild pain, and then gradually progress to severe pain [5]. If we can assess pain objectively using for example a doctorŌĆÖs diagnosis, we need to focus on these body parts and consider the transition from pain to injury. Therefore, future study is needed to investigate mechanism of pain, evaluate the pain objectively and focus on the body parts where overuse injuries often occurred.
Furthermore, the amount of playing hours was used as physical load in this study. In recent years, studies that have focused on the relationship between physical load and injuries have been actively conducted in various sports. According to the study that summarize variables used in physical load-injury investigations [26], session-rating of perceived exertion (sRPE) was most used, followed by global positioning system (GPS) and then hours. In particular, the measurements with sRPE and GPS can consider not only volume but also intensity of physical load. In handball, previous studies on the relationship between physical load and injuries used playing hours as physical load [12,13]. We also used playing hours as a variable of physical load, but it measured only the volume of load. Therefore, it is necessary to consider physical load including intensity in the future.
Conclusions
We found that pain occur frequently and that athletes continue to compete despite experiencing pain. 40% of overall pain occurrence affected the athleteŌĆÖs performance, 53.3% of which showed that performance was always limited by pains. In addition, pain occurrence is related to physical load, especially related to on-court training. Within the different body regions, it was shown that the categories of physical load related to body regions differed during on-court training.