
Introduction
Genu varum of the knee joint causes gait impairment, which then induces structural and dysfunction of the joint [1-5]. The lower limb misalignment means that loads are unevenly distributed either medially or laterally, which causes movement disorders, osteoarthritis, muscle imbalances and weakness [6] and clinical symptoms of varus and valgus can be demonstrated to negatively affect the quality of life due to physical impairments [7,8].
Varus malalignment affects the ability of a person to walk for extended times due to fatigue, and as time passes, the weight of the knee joint is concentrated unevenly, shortening the life span of the joint [9,10]. These symptoms are exacerbated while walking up or down stairs because the compression force on the knee reaches 1-2 times body weight [11] and 3-4 times body weight during running [12]. Similarly, the more the axis of the lower limb is transferred to the medial side, there is a corresponding increase in the medial loading, which is shown to be a high risk of knee osteoarthritis [5,13,14]. Therefore the management of varus knee malalignment is essential for preventing abnormal gait and reducing the probability of early onset osteoarthritis.
Gait analysis has been demonstrated to be as useful tool for the study of lower limb dysfunction, highlighting the drastic effect misalignment has on pathology of adjacent joints [1,2,5,13]. However, the majority of the studies that focus on gait and varus are mainly aimed at evaluating surgical treatment results. Additionally, these studies mainly focus on elderly patients who have already developed osteoarthritis. Whereas in this study, we plan to focus on asymptomatic females who are in their early twenties and to examine their gait to evaluate the effectiveness of exercise treatment for varus due to leg misalignment.
Today, the treatment of genu varum includes the use of a knee joint orthosis, gait pattern correction due to intentional external rotation of the foot, fascia manual therapy, and orthotics, however it is difficult to maintain lasting effects with only orthodontic treatments. Corrective exercise therapy, i.e. Pilates, to prevent and treat lower limb misalignment include a variety of mechanisms, such as stretching and strengthening to increase the varus angle of the knee joint and reduce the adductor moment of the knee joint while walking, reducing the external rotation angle of the foot, and reducing the load on the inner side of the knee joint [15]. Continuous muscle strengthening exercise is well known as an intervention for the prevention and treatment of several chronic diseases, including musculoskeletal disorders [16]. In particular, stretching, which has a positive effect on the joint load of the knee joint, helps rehabilitation of the musculoskeletal system [17-23] and elastic band exercises with Therabands, and strength exercises on unstable surfaces, i.e. a bosu, can be used to activate stabilizer muscles and help the stability of the joint [24]. As such, most of the preceding studies, especially those using Pilates showed effective improvement in static joint function by improving the knee joint spacing and hip joint motion range, which are varus knee variables due to the improvement of lower extremity muscle strength, but research on how it affects dynamic joint function during walking is insufficient.
Posture malalignment is increasing due to extended sitting periods, the use of smart phones and a general lack of physical activity [25] and this reduces core stability which leads to postural misalignments, such as genu varum [26,27]. Pilates exercise programs are well known to help increase core stability and improve posture [28,29], by an improvement in stabilization of the lumbo-pelvic region [30,19] and similarly, it is shown to improve vertebral stability [31,32]. Pilates exercise is supposed to be effective in maintaining correct posture and body balance by promoting the practitioner to recognize their body alignment and the use of muscles in their optimum lengths [33,34,35]. Ten weeks of Pilates exercise is illustrated to be effective in improving spinal alignment in the sagittal plane of 34 healthy adults [36] and 12 weeks of training improved Thoracic kyphosis in healthy adults [37]. Additionally, after 7 weeks of Pilates it was reported that dancers knee flexion and extension increased, and pelvic alignment improved [38]. As there is no known research showing the effect of Pilates on genu varum but on the trunk posture only, we were interested to examine the effect of a Pilates exercise program on genu varum of female adults not only from X-ray data, but also from a dynamic gait analysis including kinetic and kinematic data. We hypothesize that improving the trunk posture and stability will help correct genu varum alignment.
Methods
Participants
Female participants aged between 20-24 years, who had an x-ray verified genu varum diagnosis were recruited for this study, after obtaining approval from the Institutional Review Board (IRB) of Pusan National University. To participate each participant had to sign an IRB approved consent form after a verbal explanation and reading of the consent form. A total of 30 participants were recruited and randomly assigned to two groups a Pilates exercise training (PIL, n=15) and a control group (CON, n=15). Among the control group 7 dropped out due to various reasons, which left only 8 to be included in the study. The inclusion criteria were that the participants had to be females aged 20 to 24, with verified genu varum (≥10 mm [10]) and no regular participation in physical activity. Any participants overweight with a BMI greater than 25 and any other orthopedic issues were excluded. <Table 1> shows the participants demographics.
Testing procedure
Radiologic Genu Varum Evaluation
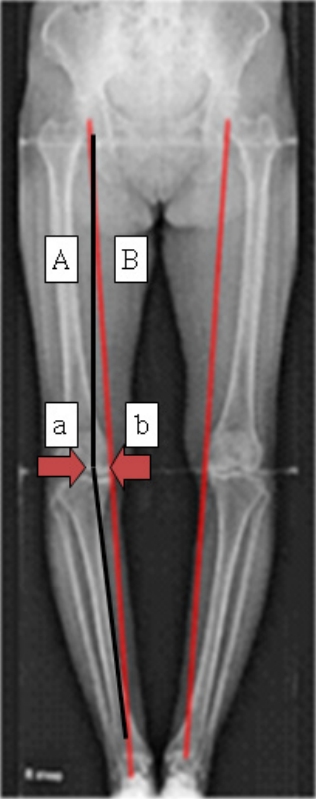
To measure and verify the genu varum the participants had their lower body x-rayed as shown in <Figure 1>. Each of the participants were instructed to stand in anatomical position, however, with their hands across their chest. The weightbearing line was drawn from the center of the hip joint to the center ankle joint. The anatomical axis was drawn from the center of the hip joint to the center of the knee joint. The distance from the center of the knee joint to the point on the weight-bearing line that crosses the knee joint was used to diagnose the genu varum <Figure 1>.
Equipment
Motion Capture
The participants’ kinematics were recorded using 6 infrared cameras (Vicon MX-T10, Oxford Metrics Ltd, Oxford, UK), and their kinetics were recorded using 2 force platforms (4060A, Bertec). For an accurate motion capture of the participants’ landmarks, the participants were instructed to change into tightly fitting sports top and shorts. For convenience of data collection 16 reflective markers (14mm in diameter) were placed on landmarks on the pelvis, thighs, shank and feet according to the Vicon standard Plug-in-gait marker set). Each of the participants had their gait recorded while they were barefooted to reduce any effects that the shoes could have on the kinetic and kinematics. The participation was requested to walk along the 8m pathway as naturally as possible while looking ahead. During the walking they were asked to try to step on the first force platform with their left foot and their right on the second force platform. Only after this familiarization period and the participant felt comfortable were 10 trials were recorded of which 5 trials were used for analysis. The dominant leg (right leg) were analyzed [39].
Ground reaction force analysis
Vicon Nexus 1.7 program was used to synchronize, record and calculate the kinematic and kinetic data. The sampling frequency was set to 1000 Hz for the signals from the force platform and at 100 Hz for the motion capture data. Each of the participant’s ground force reaction data was normalized using the participant’s individual weight. Inverse dynamics was used to calculate the joint moment forces. Left and right lower joint flexion/extension moments in the sagittal plane, the pronation moments in the frontal plane, and the internal rotation moment in the transverse plane were calculated and analyzed.
Exercise Program
The Pilates program was taken from BALANCED BODY (http://balanced body.com) mat program, which was performed 3 times a week for 10 weeks. The 60 minutes’ sessions consisted of 10 min warm-up, 40 min main exercise, and 10 min cool-down. The programs exercise intensity was set using the rating of perceived exertion (RPE) and was set to vary from RPE 11-15. Details of the program are shown in <Table 2>.
Statistical Data analysis
Descriptive data (mean and standard deviation) and mixed design (split plot) repeated ANOVA were performed using SPSS 21.0. For further analysis, independent sample t-tests were used to evaluate the statistical significances between the groups, whereas paired t-tests were used to investigate the significant differences between the pre and post intervention effects. A significance level was set to p< 0.05.
Results
Kinetic changes of the lower extremities
The results of the kinetic changes between the Pilates and control group pre and post treatment are shown in <Table 3>. For the maximum knee flexion moment, there was no interaction between timing and group, and there was no major effect between timing and groups. However, for the Pilates group there was a significant decreased according to time (p<0.05). For the maximum knee joint extension moment, there was an interaction between timing and group (p<0.05), and there was no main effect between timing and groups. For the Pilates group there was a significant increase pre and post exercise (p<0.001).
For the maximum adductor moment of the knee joint, there was no interaction between timing and group, and there was no main effect between timing and groups. For the maximum adductor moment of the hip joint, there was an interaction between timing and group (p<.001), and there was no main effect between timing and groups. There was a significant increased between the pre and post exercise (p<0.05) for the Pilates group, whereas there was a significant decreased in the control group (p<0.05).
For the maximum hip flexion moment, there was no main effect on the interaction between timing and group, and there was no major effect on the interaction between timing and groups. In the case of the maximum hip extension moment, there was no main effect on the interaction between timing and group, and there was no major effect on the interaction between timing and groups. However there a a significant decreased in the control group before and after exercise (p<0.01).
For the maximum internal rotational moment of the knee joint, there was no interaction between timing and groups, and there was no change between timing and groups. However, for the Pilates group there as a significant increase pre and post exercise (p<.01). For the maximum internal rotational moment of the hip joint, there was an interaction between the timing and the group (p<0.05), and there was also a main effect between the periods (p<.01). For the Pilates group there as a significant increase (p<0.05) but a significant decrease for the control group (p<0.05.).
Radiological changes of lower limb alignment
The results of pre and post X-ray data for the Pilates exercise and control group are shown in <Table 4>. For the alignment of the left knee joint, there was a main effect between groups (p<0.05) and between the Pilates pre and post exercise treatment (p<0.01). However, for the right knee joint, there was a significant difference between the groups but no other significant differences.
Discussion
The main results of this study were that the maximum extension and internal rotation moments were significantly increased in the exercise group compared to the control group, whereas the flexion moment was significantly decreased. As expected, there was no change in the control group. The increase in the maximum extension moment of the knee joint in the end support phase of the exercise group and the decrease in the maximum flexion moment in the middle stance phase indicates that the participants is able to absorb shock more efficiently and can stabilize with the extensor muscles during walking [40]. The maximum adductor and internal rotational moments of the hip joint were significantly increased in the exercise group, whereas the extension and adductor moments were significantly decreased in the control group. According to Moisio et al. [40] these increases in the maximum adductor and internal rotational moments in the end-stage of the supporting phase of the exercise group indicates more hip joint muscle control [40]. As for the results of the x-rays, the left leg distanced from the anatomical axis to the weight bearing line was significantly reduced in the Pilates group. However, there was a tendency of a shorter distanced from the anatomical axis to the weight bearing line in the right leg, however it was not statistically significant. Whereas there were no significant changes in the control group for both legs.
The hip extension moment is well-known as a critical factor necessary for stability and to maximize step length due to controlling the knee joint, and the maximum extension moment occurs continuously when in forward motion during the stance phase. For patients with knee hip osteoarthritis, extension moment of the knee joint tends to be reduced and this reduces the walking speed as a strategy to reduce and prevent knee pain, by reducing the load on the knee joint [41]. According to Astephen et al. [1] optimal extension moments are important as a decrease in the extension moment increases the tension of the joint tissue during walking and disrupts the normal shock absorption mechanism and becomes a risk factor that decreases the stability of the knee joint during walking. In this study, the maximum extension moment value increased in the knee joint in the exercise group showing the positive effects of the Pilates exercise.
In this study, the maximum flexion moment significantly decreased in the mid-phase of the support phase of the knee joint in the exercise group. In general, an increase in the maximum flexion moment at the knee joint maybe indicator of knee joint deformation and is associated with compensatory movement [42]. Therefore, an increase in the knee flexion moment during walking causes instability and requires a lot of energy, which causes abnormal walking. Our data showed a reduction of the maximum knee flexion moment in the Pilates group, which is thought to be a direct effect of improving the hamstring flexibility, which is the knee flexor muscle. Additionally, any reduction in the knee flexion moment is judged to have a positive effect on the knee load during walking.
Our study shows that in the transverse plane, the maximum internal rotation moment increased in the end position of the knee joint in the exercise group. Similarly, it is reported [13] that the adolescence with genu varum portrayed larger internal rotation movements at the knee joint for adolescence with knee arthritis than age matched health control participants. However, in this study, after performing Pilates exercise for 10 weeks, the female college students (age 20-24), had a reduced the internal rotational moments at the knee joint. Additionally, the maximum adductor and internal rotational movements at the hip were significantly increased at the terminal stage of the support phase. Whereas, in Stief et al. study [13] the maximum adductor moment of the hip joint was decreased in the middle and end stance phases compared to normal adolescents. These two contradictory studies highlight the need for continued investigation of the effect of different ages and abnormal developments on gait performance, especially in terms of kinetics, i.e. joint moments.
There are numerous studies showing the effectiveness of Pilates training to help pelvic alignment, stability, and treating anterior pelvic tilt [43]. Some of the reasoning of why Pilates is so affective for the pelvic stability and alignment is the concentration of the program on the deep abdominal and multifidi muscles at the lumber-pelvic region [19]. Similarly, Kang and Kim [44] states that the strengthening of the hip extension muscles and abdominals helps improve the pelvic tilt. Pilates training has also been demonstrated to be effective in improving gait function and reducing hip joint pain for elderly patients suffering from chronic fractures [30]. However, in this study the Pilates group tended to show improvements on the maximum adductor moments of the knee, maximum hip flexion and extension moments, but they were not statistically significant. Some of the reasoning why the effect may have been minimal compared to other studies is the shorter time frame of the training, 10 weeks and that the majority of the Pilates program consisted of training the core more than the lower limbs. We suggest that for future studies aimed to help alleviate genu varum, the exercise program should include a combination of both trunk and lower body exercises, including more weight bearing conditions. We also recommend that the exercise time period should be long enough for the participant to have substantial gains in strength.
Interestingly, in this study, only the non-dominant left leg of the Pilates group showed a significant decrease in distance from anatomical axis to weight bearing line of female college students after 10 weeks of Pilates exercise. It is considered that the 10-week Pilates program was effective for the left, that is, the non-dominant leg, but the 10-week exercise period not enough time for the improvement of the dominant right leg. Good alignment of the knee joint is a critical factor for spreading the loading on the articular cartilage during standing and gait, which helps prevent the degeneration of the joint’s biomechanics [6,13].
Conclusions
This study demonstrates that the Pilates exercise group had improved in the extension and flexion moment in the knee, and the adductor and internal rotation moment in the hip during walking. Moreover, this change seemed to be due to the improvement in the knee alignment verified by the X-ray data, especially for the non-dominant left leg. However, for Pilates exercise to be a more effective treatment, we suggest that future studies should include more extended training periods with the inclusion of more body weight exercises.