
Introduction
The field of tactical strength and conditioning has become increasingly popular over the past few years, and special tactical occupations, such as those of police officer, firefighter (FF), and military soldier needs efficient exercises [1]. Among these occupations, FFs require highly complexed fitness abilities such as cardiorespiratory fitness, muscle strength, endurance and etc [2]. According to the National Fire Protection Association (NFPA), a maximum oxygen intake (VO2max) value of at least 42 ml/kg/min is required to ensure the safety of FFs [3]. However, Korean FFs have shown a relatively low level of cardiorespiratory fitness (the VO2max of 63.9% of firefighters did not exceed 42 ml/kg/min) and muscle strength [4].
In a recent study, a circuit-based exercise program significantly enhanced cardiorespiratory fitness and muscle function than traditional exercise [2], and exercises targeting the muscles which were used in the fireground were effective for FFs [5]. However, there are few studies on fitness for FFs, and it appears that FF has limitations in participating regular exercises owing to the characteristics of their occupation, including shift work and emergencies [6] and most of the studies were for the foreign FFs. Thus, an effective and efficient exercise program and method to prevent injuries and cultivate work ability in Korean FFs are needed [7].
There are some new devices which appears to overcome this problem. One of these devices is a Kinect-based Mixed Reality device (KMR) that consists of a main body with a touch screen, Kinect, an image projection device, a personal computer, and a speaker. The main touch screen shows the user’s appearance and several augmented reality (AR) environments (e.g., the number of repetitions, next step, posture guide, timer, and etc). It also allows interactions with motion detection techniques in a non-face-to-face manner. Another screen by the image projection device shows images on the floor and provides a guide for movements, and displays the time, repetitions, and visual effects. This device has the benefits of providing exercises utilizing no human resources and interacting with users by detecting their movements.
The main component of KMR is “Kinect”, a camera developed by Microsoft, which is used to track the movements of twenty-five joints of the body in real time and to recognize motions. By Kinect, KMR can convert a user’s exercise performance into data in a non-face-to-face manner. It is commonly applied with a software and were used as a game, exercise, or assessment [8-12]. Another major component of this device is its mixed reality (MR) environment. MR is a combination of virtual reality (VR) and augmented reality (AR), and provides additional information by adding virtual images, while also creating an environment in which users and augmented objects can interact [13, 14]. MR has been used in various educational environments for FFs owing to its immersive and interesting factors [14]. In KMR, MR environment form an informative environment by the main screen and the image projector to users with the data of Kinect which is about the motions of the users. In the previous studies, exercise with feedbacks showed better results than none feedback exercise groups [15, 16]. Also, self-training can occur overuse injuries [9]. Therefore, this type of device can be beneficial to special occupations, such as FFs who has irregular schedule due to emergencies.
KMR is enjoyable, needs no interactions with humans, and can be enjoyed by users at any time. However, no research has been studied on this type of device that provides exercises and feedbacks at the same time. The needs for this study arise from the Kinect-based mixed reality device being future-oriented and in the spotlight, but those reliability and validity have not yet been assessed. Additionally, Korean FFs has low fitness level and does not have an appropriate fitness program to enhance their fitness abilities. In this study, we used a small number of participants with similar fitness levels to those of relatively low-fit Korean FFs because of the lack of wellness and fitness regulations in volunteer fire stations due to the Covid-19. Thus, the purpose of this study is to evaluate the intensity of a fitness program designed for low-fit FFs, and assess the reliability and validity of the Kinect-based mixed reality device.
Methods
Subjects
The reason to recruit only male in this study is due to the proportion of female FFs in the capital city of Korea which is about 5%. Also, due to the Covid-19, the fire agency reduced the employees at work so it was hard to recruit a real FFs. So, this study used a convenience sample of FFs who were in the range of Korean FFs with regard to relatively low fitness levels of VO2max (below 42 ml/kg/min) and age (20-50yrs) [4]. Total 5 male participated in this study. Participants were all students from a local university, with the following characteristics: average age (M±SD): 27.8±3.1yrs, height (M±SD): 176.2±6.2 cm, weight (M±SD): 76±10.8 kg, and VO2max (M±SD): 37.7±2.9 ml/kg/min. All participants provided written informed consent after a detailed explanation of the aims, benefits, and risks involved in the investigation. The study was initiated after explaining the experimental process to all participants in detail and obtaining their consent for participation and inspection regarding the conduct of various tests, according to the ethical principles of the Declaration of Helsinki, approved by the ethics committee of Yonsei University (IRB approval no: CR318031).
Test procedure
Using a test-retest design, five male participants undertook three trials, with 1-week washouts. Participants were asked not to drink alcohol or caffeine, avoid high-intensity exercises, sauna, and were encouraged to sleep for more than 8 hours before every visits. Inclusion criteria for the study were as follows: age between 20 and 50 years; VO2max between 28 and 42 ml/kg/min; BMI between 18.5 kg/m2 and 30 kg/m2; free of major diseases (Parkinson’s disease, cardiovascular disease, diabetes, hypertension, and hyperlipidemia); able to use a treadmill and a Kinect-based mixed reality device; on no hormonal or mental therapy; not engaged in regular moderate-to-high intensity training within the past year; nonalcoholic; on no dietary supplementation; and, non-usage of certain drugs (i.e., those influencing muscle metabolism).
During screening, the standing height (to the nearest 0.1 cm) of each participant was measured without shoes using an extensometer. Body weight (nearest 0.1 kg) was measured without shoes using a digital scale (InBody 720, InBody Co., Ltd, Seoul, Korea). Next, the participants rested for 5 min in a sitting position, and blood pressure was measured for each subject using a blood pressure monitor (BPBIO320S, InBody Co, Seoul, Korea). Aerobic fitness was assessed using a gas analyzer (Quark CPET, COSMED, Rome, Italy). The Bruce protocol was used for the graded incremental treadmill test for the screening [17]. Calibration was conducted 30 min before the test with a gas mixture and a 3-L syringe. The participants were equipped with a strap (Polar Team 2, Polar Electro Oy, Kempele, Finland), and were asked to walk on a treadmill for 1 min at 6 km/h to adapt to the device and as a warm-up. A respiratory mask was strapped onto the participant’s face, and gas leakage from the masks was checked before the test. Rating of perceived exertion (RPE) was measured using the Borg scale 6-20. This was measured after each exercise (every minute). The test was stopped when the participants met the following criteria: 1) participants were unable to continue, 2) VO2 plateau, 3) HR above 95% of HRmax, 4) RPE > 17, or 5) RER ≥ 1.10 [18]. Qualified participants were asked to visit twice. All tests were conducted at a restricted temperature and humidity in the same room.
The second and third visits were initiated after a week of washout. The participants were informed about the device before the workout, and they started the workout after they fully understood. Researchers provided login service only and comments were not allowed. Heart rate (HR) and RPE were measured during, and after the exercise session using a Polar watch (Polar Watch M600, Polar Electro Oy, Kempele, Finland) and the Borg scale. The data from the Polar watch were later downloaded using the Polar Flow website and imported as an Excel sheet for analysis.
Lactate measurement
Finger-tip lactate was measured before and after the workout using a lactate testing device (LT-1730, Lactate Pro2, Arkray, Japan). After sterilizing the finger-tip, a puncture was made using a sterile lancet. The first drop of blood was wiped away. The second drop of blood was applied to an assay strip and inserted into the lactate-testing device. The same procedure was followed for the third session.
Fitness program
The workout consisted of a circuit of 18 stations comprising resistance and aerobic exercises that used all major muscle groups and movements that would be involved in fire task (e.g., ladder climbing and carrying a hose) [5, 19]. Body weights were used for internal resisted exercises (e.g., side step, push-up, and arm walking) and two 5 kg dumbbells were used for each of the externally resisted exercises (i.e., shoulder press, deadlift, and dumbbell row). The weight of the dumbbell was fixed due to occupational characteristic of FFs which does not need periodized programs like elite athletes. So, we aimed to make one optimal fitness program. Participants were informed regarding KMR and its contents before the workout, and no other comments were provided during the exercise. Each exercise was performed for 60 s, and 15-s recovery periods were provided after each exercise to prepare for the next exercise station. The repetition and the time of the fitness program are shown in <Table 1>. Repetitions were counted by KMR using a motion-detecting camera that has standard movement points for counting. The main screen displays users on the screen with AR environments which shows the points to be reached for the counts and informed the three appropriate posture using AR environments (e.g., straightened upper body, straightened neck, etc.). For example, when “squatting” using KMR, floor images indicate a starting point using the AR environment. The exercise began when the user was at the correct starting point, and the main screen display the manner in which way to move using the AR. In this way the AR and users interact, the MR environment is generated. This was caused by human movement, which creates an AR environment by interacting with the pre-AR environment (e.g., ‘good’ indicated by blue lights and ‘bad’ indicated by red lights). Additionally, the MR environment had sound effects to encourage or provide information to the users <Figure 1>.
The table shows the components of the circuit-training. Every exercise time duration was 60 s, and the rest was 15 s. All times are presented in seconds.
Statistical analysis
This study used a test-retest design in which the same participants conducted the same exercise twice. Data were first viewed using Microsoft Excel, and all statistical tests were performed using IBM SPSS Statistics version 25.0 (SPSS, IBM Corporation, IL, USA). Descriptive statistical analysis (mean ± SD) was used to describe the variables (characteristics, HR, RPE, finger-tip lactate, and compliance). HR was expressed as a percentage of HRmax using Fox’s equation [20] and trimmed into 20 s each. To evaluate the reliability within a specific day (e.g., visit 2 vs. visit 3), the results from two repetitions from the individual trials were used for Cronbach’s alpha (> 0.9, excellent reliability; 0.7–0.9, high reliability; 0.5–0.7, moderate reliability; 0.5 and below, low reliability; and >0.7 was considered acceptable) [21] and Pearson correlation coefficient (r >.60 was considered acceptable). Statistical significance of all data was set at p < .05. [22, 23].
Results
Compliance
Five participants participated in this study. At visits 2 and 3, the participants performed 95.9±2.7% and 101.1±2.5% of the total recommended repetition, respectively.
Reliability
Through a test-retest design, excellent reliability was found for HR and RPE using Cronbach’s alpha <Table 2>. The reliability of HR was 0.967, and that of RPE was 0.969, which is near 1. According to the “items if deleted” data, every item would have a lower reliability if deleted. However, the third visit of subject number 5 showed a higher HR value than the total Cronbach a (item if deleted = 0.973), and the second visit of subject number 2 showed a higher RPE value than the total Cronbach a (item if deleted = 0.975).
The table describes the reliability of HR and RPE evaluated by Cronbach’s alpha. HR and RPE showed high Cronbach’s alpha values of 0.967 and 0.969, respectively. “Item if deleted” shows the value of each visit and the subject’s data. A score higher than Cronbach’s alpha indicates that the data has a lower value in the total data.
Validity
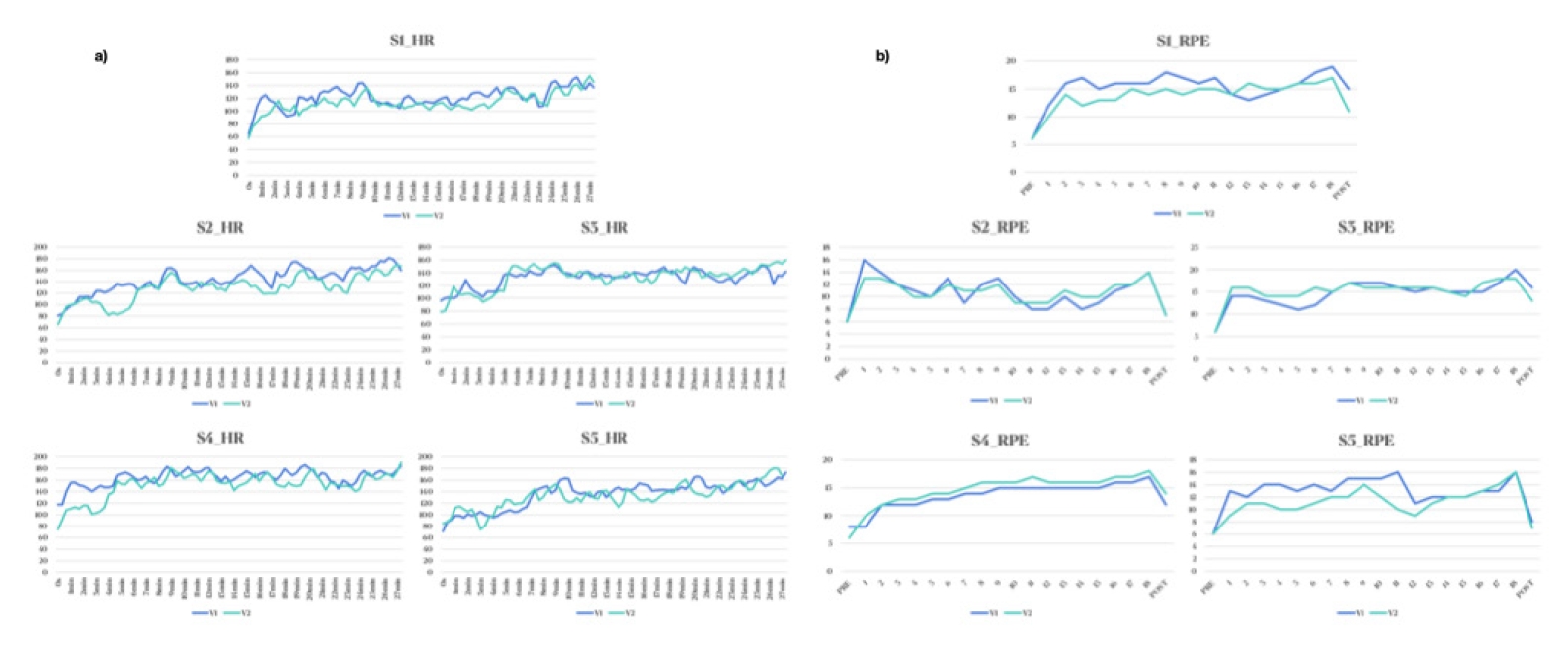
Pearson’s correlation coefficients (r) for participants 1 to 5 between visits 2 and 3 for the HR are shown in <Table 3> (r = .525 - .814, p < .001). The total data of V2 and V3 has a correlation of r = .946. The range of correlations in RPE is shown in <Table 4>, with r = .718 - .958 (p < .001). The total data of V2 and V3 has a correlation of r = .948. Which is highly correlated in both HR and RPE. Additionally, correlations can be seen in <Figure 2>; the flow chart of visit 2 and visit 3.
Intensity of the fitness program
The exercise intensities are shown in <Table 5>. The exercise intensity for RPE was in a range of “moderate-to-high intensity” (13-14: moderate, M±SD = 13.75±1.19), and that for the HR was in a range of “vigorous intensity” (70-85% HRmax: vigorous intensity, M±SD = 72.89±7.18%) [24]. Lactate showed a high value in this study (M±SD = 24.82±4.56 mmol/L). Based on these results, this fitness program was considered to be of “moderate-to-high” intensity in male participants with a VO2max range of 28-42 ml/kg/min. However, when subject number 2 in visit 2 was excluded, the intensity for RPE changed to high intensity (14-15: hard, M±SD = 14.04±0.30).
RPE, rated perceived exertion.
The intensity of the exercise program is shown above by HR, RPE, and finger-tip lactate. Heartrate and RPE were tested before, during and after the exercise and lactate were tested before and after the exercise. HR was calculated as the percentage by their maximal HR. The result shows that the intensity of the fitness program is expressed as moderate to high intensity for firefighters with low fitness level (28ml/kg/min-42ml/kg/min).
Discussion
In this study, a fitness program designed for relatively low-fit Korean FF delivered via KMR showed adequate intensity and reliable and validated results. In this study, we target the subject who has relatively low cardiorespiratory fitness due to the Korean FFs’ fitness level. Other fitness factors are also important to FFs but cardiorespiratory fitness is closely related to their work capability, cardiovascular disease, injuries, and etc [1, 7]. So, in this study, we define the fitness level to a cardiorespiratory fitness and “low-fit” as a relatively low level of fitness which means below 42ml/kg/min, a minimum of the fitness to perform their safety.
The main purpose of this study was to evaluate the reliability and validity of KMR. To our knowledge there are no studies about the evaluation of reliability and validity of the device similar with KMR which has live visual and verbal feedback with MR environment. So, we consult the main part of KMR which is Kinect. In a previous study, the validity of Kinect was evaluated using two versions, Kinect 1 and Kinect 2. Kinect 1 has low accuracy in motion detecting, which led to the development of the new version, Kinect 2. The authors compared the standard criterion of a motion detecting system with a video motion capture (VMC) system and found a similar result between Kinect 2 and VMC [6]. This result shows that Kinect 2 is a reliable and validated device for detecting motion. In another study, a software using Kinect 2 was compared with an optical motion tracking system (Vicon), which evaluated multi-joint movements, and showed high ICCvalues (>0.7) [11]. KMR uses Kinect 2 for motion detection, indicating that the KMR’s motion detection system is reliable and validated. However, KMR has several other systems which differs with the evaluation of Kinect. So, we aim to evaluate the reliability and validity of KMR itself.
To our knowledge, there are many devices that are conceptually similar to KMR, but there is no evidence for the reliability and validity of a device that generates fitness programs, detects motions, interacts with the user and has live visual and verbal feedbacks with MR environments. Therefore, we evaluated three measurements (HR, RPE and lactate level) to assess the reliability and validity of KMR. In this study, KMR showed high reliability by Cronbach alpha (0.967, 0.969) and validity by Pearson correlation (r = .525 – .814, .718 – .958; very large) using HR and RPE. By these results, KMR could be a reliable and validate device to provide exercise program.
Another aim of this study was to evaluate the intensity of the fitness program by HR, RPE, and lactate levels. HR was assessed for an aerobic fitness and lactate level was assessed for an anaerobic fitness. The mean HR (72.89±7.18%) was lower than those in previous studies on firefighting (79±6% and 79.4±5.4%) [4], [26]. However, according to the American heart association [24], the physiological response of the HR has a vigorous intensity that can enhance the ability of aerobic fitness. The duration of the circuit-training (21.5 min) is longer than that in the demanding firefighting tasks reported in previous studies (15±7 min, 17±4 min) [26, 27], which results in a larger amount of physical activity compared with higher intensity but shorter duration tasks. These results show that the fitness program designed for low-fit FFs appears to have highly intense response that can enhance aerobic fitness.
In terms of anaerobic fitness, a previous study has reported that the most demanding firefighting tasks result in blood lactate concentrations ranging from 6 to 13.2 mmol/L [28] and another study that evaluated the intensity of circuit-training for FFs [2] showed lower lactate levels ranging from 11.8±3.1 mmol/L. In contrast, this study showed peak lactate level concentration of 24.82±4.56 mmol/L. This shows that the fitness program designed for low-fit FFs has a high intensity for anaerobic systems in male who has VO2max around 28ml/kg/min to 42ml/kg/min.
Another tool of this study was the RPE of a Borg scale, it is generally used as a cost-efficient tool for evaluating exercise intensity. In a previous study, RPE showed a strong relationship between HR and blood lactate levels [29]. RPE has been used to assess the perceived intensity in FFs while performing repeated live-fire drills [30]. In this study, the mean RPE during the exercise was 13.75±6.9, which was in the moderate-intensity range (13-14: moderate, 13.75±1.19) [24]. This tool is a cost-efficient tool, but the result depends on the subjectivity of the participant and this could be the reason of the difference of intensity between HR and RPE. Further study needs to evaluate the effect of the fitness program for a longer duration.
There are some limitations of this study. First, there was only five participants in this study which was due to the Covid-19, the measurement included cardiorespiratory fitness which needs to strap mask on the participant’s face. So, it was hard to recruit the participants. Therefore, these findings cannot be generalized to all people, and a small defect could result in a relatively large effect. However, we could find the reliable and validate effect from this study. Further study should recruit more participants. Second, participants were not a real FFs. even though Korea fire agency support this study, it was hard to recruit a real FFs due to the Covid-19. Lastly, it could’ve been better to measure the lactate level during the exercise but the measurement of the lactate level of the finger needs to be sterilized and it takes time to measure. So, the measurement can induce rest period of the exercise. Therefore, we measured the lactate level as the accumulated level after the workout.
However, the field of tactical strength and conditioning has become increasingly popular over the past few years, and devices that can adjust exercises for humans with few human resources are gaining popularity. This study could further support the fitness industry and fitness environments for FFs.
Conclusions
This is the first study to evaluate the reliability and validity of the Kinect-based mixed reality device. The results showed that the KMR is reliable and validated to deliver exercises, and the fitness program in this study showed a moderate-to-high intensity, which was adequate to provoke a physiological response in relatively low-fit Korean FFs. Thus, this study indicates a fitness program designed for relatively low-fit Korean FFs delivered via KMR showed adequate intensity and reliable and validated results. Further studies will be necessary to clarify the effect of a fitness program designed for FFs using KMR devices in a large number of participants.